If thinking you’re sick can make you feel sick, is there a way to train your brain — and your body — to reverse that process and restore you to health?
That’s the central question that Tamar Koren, an MD-PhD candidate at the Technion–Israel Institute of Technology in Haifa focused on psychosomatic illness, is researching.
Professor Shai Shen-Orr, head of the school’s Systems Immunology & Precision Medicine Laboratory, is mapping how the immune system ages as people age — to the point of being able to calculate the age of someone’s immune system based on cellular data.
Professor Ron Kimmel, founder of the Geometric Image Processing Lab in the Technion’s Henry and Marilyn Taub Faculty of Computer Science, is using artificial intelligence and machine learning to train computers to analyze biopsy images of human tissue in order to determine not only whether a tissue is cancerous, but also what type of mutation it is and how much it has metastasized.
All three projects are examples of the kind of research being cultivated under the Technion’s new Human Health Initiative (THHI) — a recently announced effort to bring together teaching hospitals, different Technion departments and commercial companies to focus on solving specific health-related challenges.
“This initiative addresses world challenges that require multidisciplinary solutions,” said Shen-Orr, who is also the cofounder of CytoReason, a pharmaceutical artificial intelligence company. “We’re moving from research based on departments and faculties to being goal oriented. In addressing problems of human health, it doesn’t matter where people sit. They need to work together.”
The THHI is focused on six areas: staff and student engagement, new undergraduate and graduate educational programs, recruitment of top-notch researchers, funding, shared office and lab space for “essential meeting of minds,” and acquisition of cutting-edge lab equipment and other research infrastructure.
The new initiative dovetails with other Technion projects with outside partners, such as the university’s Bridge to Next-Generation Medicine program with Cincinnati Children’s Medical Center. That project aims to revolutionize pediatric medicine by combining the Technion’s technological prowess, including world-renowned expertise in computational science and artificial intelligence, with doctors and scientists focused on understanding and treating childhood diseases.
“The Technion believes that the time is ripe for taking the next quantum leap: addressing human health in a comprehensive, institute-wide manner,” Technion President Uri Sivan said. “The THHI represents a major intellectual and cultural undertaking in this direction. No other university in the country, and only a handful around the world, are positioned so well to take this leap.”
The idea behind the THHI is to pull people out of their comfort zones and create collaborations across units and disciplines.
“Rather than telling our investigators what they should be doing, the best way is bringing them together, and the magic is guaranteed to happen,” said Noam Ziv, who is spearheading the THHI project.
Ziv said the Technion’s prime advantage is that it’s one of the world’s few technical universities that also has a medical school.
“I don’t think you have to convince anybody that human health is a huge challenge,” Ziv said. “Our population is expanding, average age is increasing and the number of challenges associated with human health seems to be growing all the time. The coronavirus is a prime example of how things that affect one part of the world quickly affect other parts.”
During the height of the pandemic, for instance, Technion data scientists raced to improve the efficiency of PCR tests using algorithms. Biologists worked to create rapid testing kits that wouldn’t need sophisticated machines to yield quick results. Still others aimed to devised a sticker, which when placed on a mask, neutralizes viruses on contact.
The THHI extends to researching mind/body interactions.
To prove their hypothesis about psychosomatic illness, Koren and her team induced colitis in lab mice and waited for them to recover. Researchers then artificially stimulated the neurons in the brain that had become active during the bout of colitis. Inflammation re-emerged in the exact same location even though there was no infection. Likewise, suppressing memory neurons reduced the inflammation in mice who were sick with colitis.
“If, for example, you receive a text message from your friend that he has COVID and you just saw him last night, you immediately start to envision that you’re also sick. And you start to manifest physical presentations of a very similar disease: your throat itches, you start coughing, you feel weaker,” Koren said. “Studies have shown that stress or emotional triggers can initiate disease, or sometimes exacerbate a disease that’s already been diagnosed.”
Koren’s research represents a joint effort among neurosurgeons, neurologists and immunologists — the kind of collaboration THHI seeks to cultivate and which is different from traditional approaches to research.
“These kinds of collaborations have already started to develop,” Koren said. “The fact that it’s both basic science and clinical research is a novelty.”
Eventually, Koren said, her team’s work could lead to a variety of new therapies for diseases that currently have no cure, in the form of magnetic stimulation or other non-invasive therapies for patients with rheumatic arthritis, lupus, multiple sclerosis and other disorders.
“What we’re suggesting is not drugs, which also have adverse effects,” she said, “but regulation of brain activity that can alleviate their symptoms and improve their quality of life.”
The pharmaceutical industry is considered one of the important sectors growth investors should focus on because of continuous research and development of new medicines, as well as commercialisation.
The development of new vaccines and medications for COVID-19 attracted a lot of investor attention in 2020, which caused biotech stock prices to skyrocket. This trend continued until 2021, resulting in rising biotech stock prices. However, the boom gave way to a biotech bear market in late 2021. This year, the broad market has performed poorly, but biotech shares have performed even worse, underperforming the broader markets.
Investors have become less interested in risky companies in the biotech sector because of high inflation and expectations for higher interest rates. The SPDR S&P Biotech ETF (XBI), an equal-weighted index of biotech stocks, has fallen 40% since January 1, 2021, and is down 23% so far this year. On the other hand, the S&P 500 is down 13.4% YTD. However, since mid-June, biotech stocks have begun a fast-paced recovery.
While current macro trends may hurt biotech stocks in the short term, innovative technology that is well managed has the potential to do very well in the long run. Covid emphasized this extensively, which has heightened market interest in coronavirus treatment and vaccine options. Given how oversold biotech stocks have become, many of these stocks are now appearing to be bargains.
Most biotech firms research and develop multiple drugs concurrently, providing these companies with multiple revenue streams and safe investment opportunities for investors. The current challenges seen by the biotech sector could create a fantastic buying opportunity for investors looking for a stock with the potential for significant long-term growth.
Given all of the above, here are 4 promising biotech companies to consider.
Intellia Therapeutics Inc (NTLA)
Intellia Therapeutics, founded in 2014, is a leading genome editing company that develops curative gene-editing treatments. The company’s programs include the treatment of transthyretin amyloidosis, hereditary angioedema, and acute myeloid leukemia; and proprietary programs focused on developing engineered cell therapies to treat various oncological and autoimmune disorders. Intellia also has licensing and collaboration agreements with various research institutes.
The company continues to make excellent progress with its clinical trials and is expected to present early-stage interim data from a couple of trials and make a major regulatory filing by the end of 2023. In recent financial results, Intellia reported positive progress in both the cardiomyopathy and polyneuropathy arms of the landmark Phase 1 study of NTLA-2001. The stock is down 45% YTD presenting a good time to add this stock to a growth investor’s portfolio as the positive events expected in the coming quarters might drive its stock higher in the coming months.
BioMarin Pharmaceutical Inc (BMRN)
BioMarin Pharmaceutical, Inc., founded in 1997, is a biotechnology company that engages in the development and commercialization of therapies for people with serious and life-threatening rare diseases and medical conditions. Its commercial products include Vimizim, Naglazyme, Kuvan, Palynziq, Brineura, Voxzogo, and Aldurazyme. The company’s pipeline includes Valoctocogene Roxaparvovec (Roctavian) which is in Phase III clinical trial for the treatment of Hemophilia A; BMN 307, an AAV5 mediated gene therapy which is in Phase 1/2 clinical trial; and BMN 255 which is in Phase 1/2 clinical tria for treating primary hyperoxaluria.
The company recently announced its Q2 earnings which surpassed analyst estimates. BioMarin reported $533.8 million in sales, up 6% Y/Y. Further, Voxzogo for achondroplasia (dwarfism) reported sales of $34.4 million. An estimated 446 children were being treated with commercial Voxzogo globally, compared to 284 children in Q1 FY22.
The stock is up 4% YTD and is expected to perform well in the long-term with the company’s commercial sales for Voxzogo in Japan and Australia expected to begin in Q3. BioMarin also expects that Roctavian will be approved in Europe in Q3, with FDA resubmission planned for September.
NurExone Biologic Ltd. (NRX.V)
NurExone is working on a treatment for traumatic central nervous system damage based on groundbreaking biological extracellular vesicles (E.V.) technology. This startup is developing ExoTherapies, in which exosomes are loaded with healing molecules, and an easy-to-administer delivery system to change the way traumatic spinal cord injury (SCI) is treated around the world. According to the World Health Organization, the estimated global SCI incidence is 40 to 80 new cases per million population per year.
NurExone’s first ExoTherapy, ExoPTEN, has shown very promising results for spinal cord injuries during animal studies. It promoted exon-growth functional recovery, or nerve regeneration. This suggests that NurExone’s groundbreaking and proprietary exosome-based therapy has the potential to provide a much-needed, functional-recovery providing treatment for SCI.
The company holds a worldwide exclusive license agreement with the Technion, Israel Institute of Technology in Haifa, for the development of technology, clinical trials, and commercialization. Nurexone (NRX.V) is now listed on the TSX Venture Exchange, following the completion of a Reverse Takeover Transaction.
Israel is home to more than 400 active biotech startups that have shown remarkable growth by leveraging advanced technologies. The country is known for investing the highest percentage of its GDP in R&D encouraging academic centers and research groups to develop breakthrough treatments. Given the availability of resources and support, alongside the fast-growing industry NurExone is pursing, the company is primed to experience significant growth in the coming years.
Vertex Pharmaceuticals Incorporated (VRTX)
Vertex, founded in 1989, focuses on the discovery, development manufacturing, and commercializing of breakthrough small molecule drugs for serious diseases including cystic fibrosis, infectious diseases, autoimmune diseases, and neurological disorders. The company reported strong second-quarter results with product revenues up 22% Y/Y to $2.20 billion.
The stock is up 24% YTD. Given the company’s recent pipeline development, the stock has more upside potential. Vertex’s CF (cystic fibrosis) drug TRIKAFTA recorded strong performance in the United States. As a result, the company expects the demand for CF drugs to remain high additionally driven by the launch of KAFTRIO outside the United States. Vertex has completed the Phase 3 study of TRIKAFTA/KAFTRIO in children 2 to 5 years old and expects to submit global regulatory filings for TRIKAFTA/KAFTRIO in children 2 to 5 years old this year.
Vertex has also filed a Supplemental New Drug Application (sNDA) with the U.S. Food and Drug Administration (FDA) and a Marketing Authorization Application (MAA) with the European Medicines Agency (EMA) for the use of ORKAMBI in children 12 months to less than 24 months old.
Conclusion
Biotech stocks have started to recover with some big players reporting positive growth in the recent quarter. Investors who add the right biotech companies to their portfolio now will be able to reap lucrative rewards in the long run when the bear market eventually subsides.
Researchers at the Israel Institute of Science and Technology are making great strides in how the disease is both detected and treated
Technion professors and graduates are continuing to make significant contributions in the field of cancer research.
Professor Yuval Shaked, along with startup, OncoHost, has created a blood test that will allow doctors to provide personalised treatment plans to cancer patients, Ibex Medical Analytics, headed up by Dr Daphna Laifenfeld (who researched it during her time at the university), has created an Artificial Intelligence-based cancer diagnostic software, while NanoGhost, co-founded by Professor Marcelle Machluf, is another technology “that targets cancer cells with modified adult stem cells loaded with medicine.”
Having already raised $5 million, NanoGhost – which innovatively delivers cancer medicine directly to tumour cells, allowing the potency to be reduced by a factor of a million – has been treating pancreatic, lung, breast, prostate and brain cancer successfully in mice.
Professor Machluf says: “This integration turns the NanoGhost platform from a ‘taxi’ that delivers the drug to the target into a ‘tank’ that participates in the war.
“The integrated platform delivers the drug to the tumour and enables a significant reduction in drug dosage yet still does the job. We also showed that our method does not harm healthy cells.”
NanoGhost is on track to begin clinical trials in 2023.
The university team has tested its research on mice in a novel trial
A team of scientists from Technion – Israel Institute of Technology has used genetically engineered muscle tissue to cure mice of type 2 diabetes.
Muscle cells are among the main targets of insulin, which is supposed to absorb sugar from the blood. However, in type 2 diabetics, this ability is reduced.
Up until now, restoring the metabolic activity of muscles has just been an unexplored idea. Now, however, the theory has been proven – thanks to Professor Shulamit Levenberg, Dean of the Faculty of Biomedical Engineering at the Technion and doctoral student Rita Beckerman.
Isolating the muscle cells and engineering them to be metabolically functional before transporting them back into the abdomen of the diabetic mice led to the now-healthy cells absorbing sugar correctly and improved blood sugar levels – both in the abdominal muscles and elsewhere in the body.
The mice remained cured of diabetes for the entire four-month period which they were observed.
Professor Levenberg said: “These cells worked hard and absorbed glucose, and also secreted factors that systematically affected the metabolism of the mice.
“The approach can be used to rescue mice from their diabetic situation, and now we hope to be able to use it in the future as a treatment for humans.”
“It’s such a novel approach that we really didn’t know what to expect, but we were extremely happy with the result”, Beckerman added.
“This could potentially, in the future, give human patients with Type 2 diabetes the possibility of having an implant and then going for a few months without taking any medications.”
The research is published in the peer-reviewed Science Advances journal.
Diabetes currently affects 4.7 million people in the UK, according to Diabetes UK – 90% of which will have type 2. Type 2 diabetes can lead to long-term complications such as heart disease, stroke, kidney failure and blindness.
This Israeli startup finds key ingredients in nature that are also found in breast milk
The ingredients that make mother’s milk the best possible thing for a baby will now be available for grownups.
Israeli food tech startup Maolac uses an algorithm that matches the key proteins in breast milk with alternative sources found in mushrooms, algae, and plants.
Everything that baby benefits from — protection against illness, anti-inflammatory qualities, and nutrition — will be utilized in a superfood for adults, Maya Ashkenazi Otmazgin, and biomedical engineer and the CEO for Maolac, tells NoCamels.
“We created an algorithm that can actually look at all the proteins inside breast milk and mix and match the key proteins responsible for different functionalities and then find them in alternative sources in nature, like mushrooms, algae, and plants,” she says.
Maolac is also said to be the first company in the world to identify and extract functional proteins from bovine colostrum, a nutrient-rich milky fluid that comes from the udder of cows in the first four to five days after giving birth, which is 95 percent equivalent to those found in breast milk, according to the firm.
Bovine colostrum produced by baby calves should not go to waste. Image by Erdenebayar Bayansan from Pixabay
Extra milk from calves– as much as 20 liters per cow — is thrown away after getting a certain amount from each one. “If we look for it, we will see 5 billion liters of bovine colostrum that the dairy industry does not use,” Ashkenazi Otmazgin says.
“The idea of transforming the first, nutrient-rich milk of cows that have just given birth into a source for human protein is a stroke of pure genius. Billions of liters of bovine colostrum are discarded each year. Maolac takes this waste and creates a product of huge potential benefit to millions at a time when the world is desperately searching for new sustainable sources of protein. The company is a perfect example of the circular economy in action,” said Jon Medved, CEO of OurCrowd, which has invested in the company.
Nursing vision
Otmagazin had the idea to create a superfood using nutritional ingredients found in breast milk while experiencing “the magic” of nursing her first child. She realized she wanted to harness the benefits of that breast milk for adults.
“I told myself – this is the ultimate superfood for mammals,” she says in a conversation with NoCamels during a short break between a hectic day of meetings. “There are different functionalities that breast milk can provide for a small human being and I realized we could leverage all the goodness to create something new inspired by a formulation that created the human species and actually brought us to where we are,” she says.
In 2018, Ashkenazi Otmazgin joined forces with Eli Lerner and immunity expert Dr. Ariel Orbach to form a food tech startup. The company just raised a $3.2 million seed funding round led by active crowdfunding platform OurCrowd with participation from The Kitchen FoodTech Hub founded by the Strauss Group, The Food Tech Lab, VentureIsrael, NEOME, and Mediterranean Towers Ventures.
Studies have shown that there are numerous benefits to breastfeeding a baby that both protect against illness and positively impact health and child development. According to the Cleveland Clinic in Cleveland, Ohio, USA, breast milk provides abundant and easily absorbed nutritional components, antioxidants, enzymes, immune properties, and live antibodies from the mother that attack germs and protect the baby from illness.
Maolac superfood products. Courtesy.
Maolac’s technology relies on a bio-convergence platform for the discovery of proteins based on machine learning and natural language processing search algorithms. The company identified more than 1,5000 known bio-active proteins in human breast milk and over 400 homolog proteins in bovine colostrum, and have since created thousands of human functional milk protein mixtures using similar ingredients found in plants and mushrooms, and other sources found in nature.
Ashkenazi Otmazgin stresses that the alternative sources must come from nature. “We don’t make them in a lab or genetically modify our mixtures.”
Maolac’s active ingredients work like breast milk to directly target specific body function, traveling through the bloodstream or gut to produce higher overall efficacy at lower dosages, a statement from Maolac said.
One of the ingredients has anti-inflammatory properties and is part of the first Maolac product line for humans. It will target athletes to reduce muscle strain and improve recovery time. The product will also target the elderly to support living and improved mobility. It will form the basis for the next generation of gut health solutions for humans and pets to help prevent severe cases of gut inflammation.
The second ingredient will be a part of products creating the next generation of probiotics, according to Otmazgin. It will contribute to a better digestive system to reduce inconvenience due to stress in the gut, irritable bowel syndrome (IBS), or other conditions
Maolac will use the seed funding they just raised to build a state-of-the-art facility that will feature small-scale production capabilities. The facility will also be able to create analytics and samples for customers and clinical trials.
The Maolac team. Maya Otmazgin is in the center. Courtesy.
Ashkenazi Otmazgin tells NoCamels that the startup is in advanced discussions on joint development agreements with several leading Israeli companies in the food and supplements markets. It is also in talks with several of the world’s leading dairy protein producers and global dairy, ingredient, and supplement companies.
“We have several contracts on the table with potential global manufacturers that will produce for us. Our intention is to go global,” says Ashkenazi Otmazgin, citing both the US and Europe.
“We want to be the next generation of smart ingredient companies that create precision proteins for the food supplements and cosmetics industries with a portfolio of products with different functionalities,” says Ashkenazi Ashkenazi Otmazgin, “We want to bring active ingredients in small doses that won’t have an influence on taste, texture, or colors of existing food products, so people will love to consume those products.”
Ashkenazi Otmazgin also admits that in the future, the company will go to other markets, like the baby formula market. “Not full formula, but functional ingredients for the industry,” she adds.
For now, though, the focus is breast milk.
“There are so many companies that work in the alternative space and don’t look at breast milk — there is something quite repulsive when you talk about it. But adults can take real advantage of it,” she says.
Two-minute AI profile saves physician from time-consuming trawl of medical records
The average doctor’s appointment lasts about 20 minutes — 30 if you’re lucky. The physician sees dozens of patients, many with complex histories and taking a range of medications. Every detail is important, but there’s no way a doctor can keep track of it all.
Enter Navina (“Together we Understand” in Hebrew), a platform that uses AI to present a doctor, with an entire in-depth medical history that they can read and digest in two minutes.
It presents them with indications of risk factors, illnesses, and treatments of a patient, in an easy-to-read patient profile that can be accessed through a smartphone app. So they no longer need to trawl through a mass of records going back months and years from different hospitals and different specialists.
The company was founded by two former intelligence officers who revolutionized the use of AI during their time in the IDF to present military commanders with the data they needed, when they needed it.
They are now adapting that model to help busy doctors who need to have all relevant data at their fingertips the moment their patient walks into the surgery.
Navina says it turns “chaotic data into actionable patient portraits”. The portrait replaces disorganized patient data with a logical grid that makes it possible for a primary care physician to access a patient’s medical records within seconds.
Navina’s patient portrait provides a one-page summary with critical information from many sources, including images, emails, and faxes that are hard for physicians to find on their own.
The team teaches the machine how to extract the proper data no matter what the source. To do this, Navina developed NLP (natural language processing) models which extract and structure the data through deep learning. with special codes for specific terminology.
Ronen Lavi, co-founder and CEO of Navina, compares the profile to what happens when you do a Google search on a person, where clicking to search will get you a page that is a roundup of the person with a photo, biography, information about life experiences, and articles correlated with the person. Similarly, Navina would present a contextual summary of a patient’s most pertinent medical information so that physicians can understand their health status.
Navina presents the doctor with a two-minute in-depth patient profile. Deposit Photos
“We built algorithms to do two main things. First, you have a lot of unstructured data — a lot of text. In a process called entity extraction, we extract all the right relevant codes out of the text, all the labs, all the meds, all the problems, all the diagnoses, through machine learning (ML) capabilities. Then, we build a knowledge graph that links all the data,” he tells NoCamels.
“For a problem like blood pressure, [the profile] will show you the right medication, the right consult notes, the right lab tests, everything is correlated and explained to the physician. That’s the two main things we’re doing behind the scenes,” he says, noting that it’s about taking all the information, doing a correlation, and then creating a link that gives you a contextual understanding of your subject.
“What we saw was one of the main problems of physicians. They can address one or two problems — maybe three — if they know them in advance,” Lavi adds. “Five minutes before having to leave, the patient remembers – ‘Oh, hey, I have to ask you about this medication. I have to ask you about the new problem I have. I have to ask you about my family — and the physician hates this. The patient also hates it because they get the answer, ‘Sorry, my friend, I can’t deal with this right now. I have to go to the next meeting. And the patient doesn’t get the full attention he needs.”
The Navina app is currently being used by some 1,500 physicians and at leading clinics across the United States. The company is also marketing the product to health providers and risk adjustment teams , that predict future health care expenditures of individuals based on diagnoses and demographics.
Cutting through the clutter of patient data
The healthcare industry has amassed a huge amount of data over time, which has quickly become disorganized and difficult to manage. With so much data to analyze so quickly, health professionals often turn to AI to organize and interpret the data for improved insights.
This isn’t easy, Lavi tells NoCamels. In fact, it’s “complicated technology,” which explains why it hasn’t been done before. But Navina has a number of AI and medical experts on its team, including two co-founders with experience in the elite 8200 unit of the IDF, where they focused on bringing AI from theory into practice.
Lavi spent 24 years in 8200 and at the Prime Minister’s Office, where he established and led the AI Lab of Israel’s Military Intelligence, which collaborates with leading tech companies and academia to develop cross-functional platforms that provide insight into challenging data. Shay Perera, CTO at Navina spent a decade in elite intelligence units, where he was involved in R&D and held leadership positions. He also has a Master of Science in electrical engineering from the Technion with a specialty in machine learning.
Perera says a relative of his was diagnosed very late with cancer due to mistakes by the family doctor and his condition deteriorated as a result. The pair realized GPs were missing out on many critical diagnoses because they couldn’t absorb the volume of patient data they had to deal with.
The Navina team behind the app that turns chaotic data into clear information for doctors. Courtesy
Lavi and Perera were responsible for one of the greatest revolutions that took place in 8200 and later in the IDF – the smart data revolution that is presented to commanders in real-time. The two built the AI / ML-based information systems of the cyber units that processed data and upgraded the capabilities of cyber commanders and won a National Security Award for their efforts in 2018.
After being released from the army, the two used their knowledge and expertise in data, AI, and machine learning to make a difference in people’s lives. For Naviana, founded in 2018, the two replicated the data model they built in the IDF to implement it in health institutions around the world.
“I think the gain for the patient is very obvious,” says Lavi, “They want to get everything to be addressed. And the physician should be with the patient, not with the computer. And that’s what Navina allows them to do because everything’s summarized for you in two or three clicks.”
“Navina is disruptive because it’s one of the first digital health applications that I know of, which the physician is actually willing to use. It’s not a burden. The machine behind the scene does a lot of stuff for them that allows them to understand the patient very easily. And every time I say that, people ask how did nobody think about it before and why hasn’t it been done.”
These Israeli companies use mobile phones to gather and/or transmit health data and keep tabs on chronic conditions.
Social entrepreneur Ariel Beery and optics expert David Levitz had the inspiration to use the built-in camera of a smartphone to screen for cervical cancer — the fourth most common cancer affecting women globally and the second most common cancer for women in low-resource settings.
“More than five billion people around the world have access to mobile phones, but not to a physician,” Beery told ISRAEL21c in 2014, when the prototype was being piloted in five countries.
“We can do what a $100,000 device can do on a mobile phone, with 10 times better magnification than using just the naked eye, raising diagnostic accuracy significantly.”
Today, the EVA point-of-care device from MobileODT is used by primary care providers in 30-plus countries to conduct specialist-level visual screenings for thousands of women.
Ariel Beery, general partner of CoVelocity Health. Photo by Erin Kopelow
“MobileODT was the first company to build an FDA Class 2 medical device — a regulated medical device that replaces an existing medical system — around a mobile phone,” says former MobileODT CEO Beery, now general partner at CoVelocity Health, a strategic commercialization partner for medical technologies.
Since then, many other companies have harnessed the mobile phone – either to help healthcare professionals gather data (as with MobileODT) or to help patients transmit data from home to the practitioner and facilitate communication during a remote exam.
“There are a number of reasons why mobile phones make sense to be the core platform for a medical device,” says Beery.
“The first one is that every single person on the planet knows how to use one. And that is so important, because training and onboarding for a medical device is very difficult. When you have something based on a mobile phone platform, it’s relatively easy for the practitioner to watch a few tutorials and very quickly start using the device. That’s not the case with anything else, and it’s super important because then you can expand into rural areas and low-resource settings efficiently.”
There are other advantages of using smartphones for healthcare.
“From a regulatory perspective, most mobile phones in the market have received both electrical testing and broadcast certificates. Wi-Fi is intermittent around the world, but when you have a SIM card and a device that will be connected or integrated with medical information systems, a mobile phone shortcuts a whole host of regulation and registration — things that are really hard and expensive to do,” Beery adds. “For any [medical] device that requires communication, mobile phones already have all that already baked in.”
Below are descriptions of 13 companies using the smartphone as a basis or adjunct for smart healthcare.
MobileODT
Photo of the EVA system courtesy of MobileODT
Beery and Levitz originally envisioned EVA as a colposcope addon for the healthcare practitioner’s own phone. The current version instead has a dedicated Samsung J530 built in for all-in-one visualization, documentation and teleconsultation.
“We learned that there’s a big difference between things that assist a health worker in decision-making or communication functions, where using their own mobile phone makes sense; and information-gathering or diagnostic functions, in which case a dedicated mobile phone makes sense,” Beery explains.
“Diagnostic functions require your device to touch the patient. That brings up issues of security and sterilization. Also, a dedicated phone doesn’t have the same wear and tear and memory issues that you have with someone’s personal phone and doesn’t conflict with their images and WhatsApp and what have you.”
The EVA product line now includes separate devices for cervical cancer screening, cervical examination and sexual assault forensics. It’s also used to train clinicians in colposcopy; telecolposcopy or remote colposcopy.
Binah.ai
Remotely or onsite, Binah.ai’s video-based solution provides medical-grade vital signs measurements — heart rate, heart rate variability, mental stress level, oxygen saturation, respiration rate and more — within 2 minutes via a video of the patient’s upper cheek taken with a smartphone, tablet or laptop.
The signal processing and AI technology compensates for motion and imperfect lighting, and supports any age, gender and skin color. It can even detect subtle changes that might otherwise go unnoticed. Binah.ai works with healthcare, insurance and wellness industries in several countries.
Binah.ai is headquartered in Ramat Gan with offices in Maryland and Tokyo.
Healthy.io
This Tel Aviv-based startup, founded in 2013, leverages the image-processing capability of any smartphone camera for four at-home Minuteful medical tests – kidney function, wound management, urinary tract infection and urinalysis — whose results are transmitted to the clinician instantly.
Healthy.io’s partners in the US and UK include, among others, the National Kidney Foundation, the National Health Service, Modality and the Boots chain. The company recently acquired its American competitor, Inui Health, for $9 million.
K Health
K Health, billed as “healthcare without the system,” provides 24/7 phone access to board-certified doctors in 48 US states for $29 per month (no insurance necessary), where it has some 6 million users. The entire intake process is done on the smartphone, and users text K Health when they are free for a consult.
K Health provides 24/7 access to physicians as well as a free symptom checker. Photo courtesy of K Health
Members can download a free AI-powered symptom-checker app and obtain on-the-go prescriptions and refills. Primary care, urgent care, mental health and pediatric care (as well as Covid-related services) are all included. K Health is based in New York with development offices in Tel Aviv.
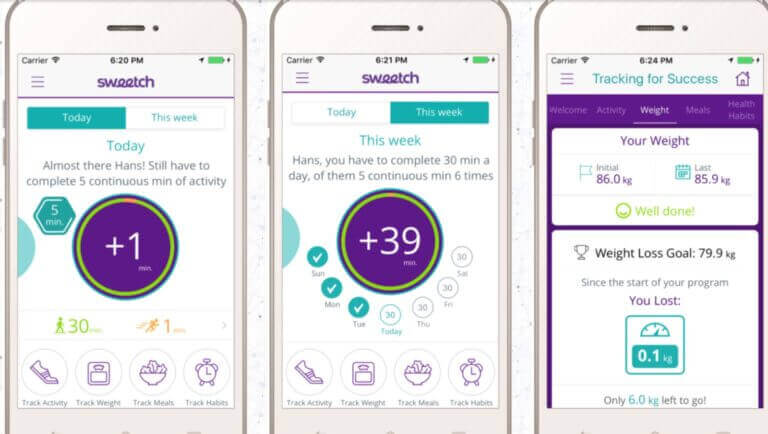
Sweetch
Sweetch provides a personalized digital coach for preventing and managing chronic diseases. Image: screenshot
Sweetch is a mobile based digital coach providing personalized recommendations for preventing and managing chronic conditions, generated from analysis of millions of datapoints on the individual’s smartphone and other connected devices.
In addition to the Sweetch app, the technology is available as a white-label app or as an SDK to be integrated within an existing app. Headquartered in Tel Aviv, Sweetch is used in countries across the world.
Montfort
Montfort bridges technology and neurology, turning any standard smartphone into a personalized neurological medical testing device.
Using smartphone sensors and AI, Montfort’s EncephaLog app provides FDA-cleared digital neurological tests for early diagnosis of conditions such as Parkinson’s disease, Huntington’s disease, anxiety, depression, post-Covid-19 neurological symptoms and more.
In the app, patients see the specific tests prescribed with reminders about when to take the tests and instructions in the patient’s preferred language. Montfort is used in more than 10 countries.
The tests measure parameters in three dimensions — motor (such as balance, gait, tremor), cognitive (memory, response time, pattern recognition) and mood indicators. It merges those measures with a fourth dimension of physiological records (genetics, brain scans, data from wearable devices) for a holistic picture.
Nonagon
Nonagon, backed by Phillips and Teva, has FDA and CE approval for its smartphone-based telemedicine device.
Four embedded sensors interface with the user’s smartphone to provide readings of nine common tests required for primary medical care: a stethoscope check (lung, heart and bowel sounds), otoscopy of the ear, oximeter (pulse rate and saturation), thermometer (body temperature), and a throat and skin test that uses the smartphone’s camera.
The device works with patients as young as two years old. The clinical data is sent in real time to the physician, enabling near immediate diagnosis, referral or prescription. Formerly known as MyHomeDoc, Nonagon is based in Caesarea with offices in New York.
TytoCare
This company’s award-winning TytoHome remote exam device ties in with the user’s and physician’s iOS or Android smartphone (or other device) via an app that allows the practitioner to control and guide the entire exam in real time.
For example, the clinician can take control of the stethoscope adapter to listen to lung and heart sounds or use the otoscope adapter to check ears for infection. After confirming a diagnosis, the clinician can send further instructions or a prescription.
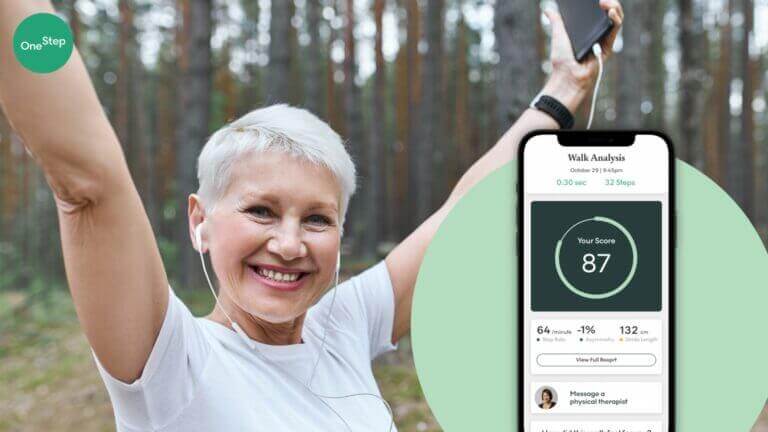
OneStep
Photo courtesy of OneStep
OneStep of Tel Aviv developed an app-based physical therapy platform providing comprehensive gait analysis using only smartphone sensors.
The user needs nothing more than a smartphone nearby while doing the prescribed exercises. The app gives a detailed assessment of walking and overall mobility and allows physical therapists to communicate and provide effective treatment to patients 24/7.
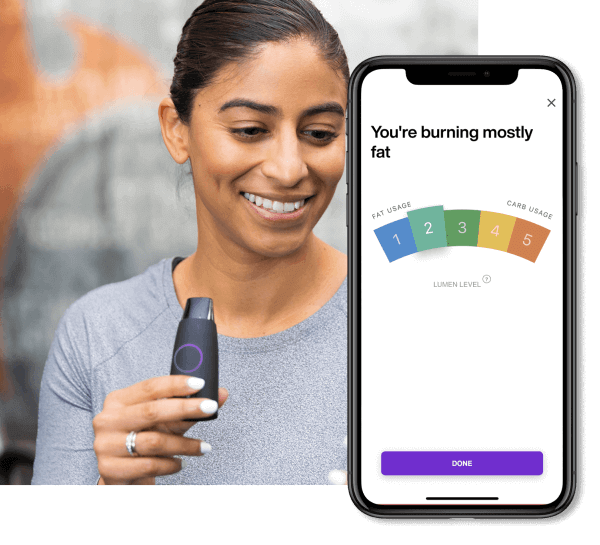
Lumen
Lumen’s handheld device allows users to analyze and monitor their metabolism with their smartphone. It reveals the body’s current source of energy — fats or carbs — on a scale of 1 to 5, based on the respiratory exchange ratio.
Image courtesy of Lumen
The score helps users adjust their daily diet and physical activities accordingly: Low-carb days decrease the insulin spike, improving insulin sensitivity and enhancing mitochondrial function, while high-carb days ensure the body’s ability to use carbs for energy and keep hormones in balance.
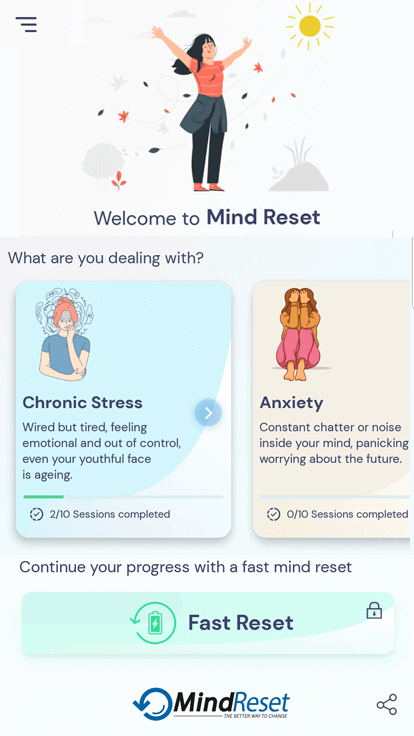
MindReset
This app built on eye-tracking technology from Jerusalem-based Umoove helps thousands of users “reset” their response to depression, trauma, anxiety, stress and other emotional triggers.
Image courtesy of MindReset
An audio guide takes the user through each daily two-minute session of a 10-day program tailored to specific conditions. The eye tracker on the phone’s camera detects patterns in eye movement that indicate a stress trigger. Users are directed to do certain tasks with their eyes that interrupt the pattern and thus create a therapeutic effect by clearing the triggers.
The unique method behind the app was published last November in the journal Frontiers.
Yitzi Kempinski, founder-CEO of Umoove and CTO of MindReset, says results are so encouraging that the company is researching other ways people can use the app, such as for work burnout or emotional barriers to learning.
Neuralight
Using ocular metric data captured with a standard webcam or smartphone, this Tel Aviv- and Texas-based startup is building an AI-driven platform to accelerate and improve drug development and patient monitoring, as well as introduce precision care for patients with neurological disorders.
A physician records a five-minute video of a patient’s eye movements. Neuralight’s imaging tools clean up the video, then artificial intelligence and machine learning decipher what’s behind the eye movements.
The concept is based on scientific studies over the past 20 years showing correlations between various oculometric measures and the neurological status of patients suffering from a range of neurodegenerative and psychiatric disorders.
Cordio Medical
Cordio Medical’s HearO technology can sense fluid accumulation related to congestive heart failure through a patient’s speech and send an alert. This noninvasive monitoring solution is based on true speech signal processing augmented with machine learning.
The user speaks into a smartphone app whose algorithms allow near real-time monitoring and early detection of condition deterioration. The system is patient-tailored, constantly learning the patient’s voice. HearO noninvasively.
The company recently raised $18 million and aims to enter the US market in 2024.
Technion-patented technology enables monitoring and early identification of changes in the condition of respiratory patients at home or in hospital.
The Jerusalem Post has partnered with ExitValley, a digital platform that enables anyone to invest in Israel’s start-up ecosystem and share in its success. In this article, we are pleased to introduce NanoVation-GS, an Israeli company that has developed a first-of-its-kind nanosensor-based technology for monitoring and managing chronic respiratory conditions at home or hospitals while reducing hospitalizations.
The patented technology was discovered at the Technion and is undergoing clinical trials in Israel and the EU. “The technology enables surveillance and early identification of changes in the patient’s condition. In addition to reducing hospitalizations, it is also expected to reduce their duration”, says the company’s CEO and co-founder, Dr. Gregory Shuster, Ph.D.
NanoVation-GS has developed a unique technology for monitoring patients with chronic lung diseases, with an emphasis on obstructive diseases such as COPD – Chronic Obstructive Pulmonary Disease, which enables early detection of worsening of symptoms and helps reduce prolonged and frequent hospitalizations by allowing the patient to receive appropriate early treatment. “The device is designed to measure important respiratory parameters without any discomfort or effort needed by the patient,” says Dr. Shuster.
NanoVation company’s CEO and co-founder, Dr. Gregory Shuster, Ph.D. (Credit: NanoVation)
The development is based on advanced nanosensor technology, which for the first time allows accurate monitoring of changes in respiratory function without any discomfort or effort from the patient, and is particularly sensitive to fluctuations and changes in several critical respiratory parameters. “One of the things we identified was the gap in technologies related to respiratory monitoring. When you look at monitoring in cardiology, for example, there are much broader tools than in respiratory monitoring,” Dr. Shuster explains.
The solution provides the ability to manage chronic respiratory diseases via the cloud, allowing doctors to review data from any location, during hospitalization, and during the follow-up period at home, which also enables the creation of “big data”-bases of all relevant information. “The system is simple to use at home without any need for professional assistance or in a clinical environment. It operates in a non-invasive method, measures normal and effortless breathing, and uses exclusive biomarkers which were identified by the company’s technology,” Dr. Shuster adds.
“The system is simple to use at home without any need for professional assistance or in a clinical environment”.
Dr. Gregory Shuster
NanoVation-GS was founded at the Technion by a leading experienced team, including Dr. Shuster- founder and CEO and senior researcher in nanomaterials and materials engineering, and Prof. Hossam Haick, founder and CSO, a leading researcher and expert in nanotechnology. The company has an exclusive license for its first patent from the Technion and two additional patents owned by the company, which are in the registration phase.
NanoVation-GS has been granted a prestigious development grant by the European Innovation Council (EIC), which only supports start-ups identified as companies with a significant impact and groundbreaking technology. In addition, the company has previously received grants from the Israel Innovation Authority. “Breathing monitoring technologies today can be divided into two groups,” says Dr. Shuster. “One is the technologies that measure normal breathing, which are not invasive or annoying to the patient, but the data collected is limited to the parameter of breathing rate only.
Nanovation Technology (Credit: NanoVation)
“The second group provides a series of respiratory parameters, but it requires the patient to perform certain breathing maneuvers. This is a complicated test for the patient to perform at home. It is bothersome, unpleasant for the patient, and the doctor who receives the data cannot know whether the test was performed properly, because he did not see the patient do it.
“What we do is combine the benefits of these two worlds,” says Dr. Shuster. “On the one hand, our measurement takes a few minutes, during which the patient puts on the sensor and does nothing extra. On the other hand, the data we extract provides a series of respiratory parameters, which are very relevant to changes in the disease condition. All this in one simple test, which can also be done routinely at home. The patient cannot get an incorrect measurement, because all he has to do is breathe naturally.”
The company’s SenseGuard product has been tested so far in successful clinical trials at leading partners in Israel and around the world, including Halle-Saale University Hospital in Germany, Nicosia Lung Center in Cyprus, and in Israel at Ichilov Medical Center, Poriah Hospital, Nazareth Hospital, Rambam and Barzilai Hospitals and the Galilee Medical Center.
NanoVation-GS has completed all procedures needed for obtaining the necessary regulatory approvals for medical devices, including CE certification and international ISO standards. The company will work to update its existing CE certification to the new standard (MDR), while also planning to obtain FDA approval at a later date. NanoVation-GS is ready to start marketing activities in Europe towards entry into the COPD monitoring market, which is its first phase destination market, and later will turn to other territories and examine further commercial and clinical applications.
“Right now, we are focusing on the medical field, looking at chronic respiratory patients, but plans for the future are varied,” Dr. Shuster concludes. “The use of our technology can also be extended to other respiratory and non-respiratory diseases, sleep monitoring and even entering the field of wellness, by measuring and helping to manage the level of stress, assisting with breathing exercises in yoga and more.”
The Technion has received its first human MRI research scanner made by Siemens. The device will operate within the framework of the May-Blum-Dahl Human MRI Research Center in its own 200 square meter facility in the Technion’s Joseph Center for Industrial Research.
The new Center, operated by the Faculty of Biomedical Engineering, will be used by researchers, professors, and students to carry out interdisciplinary research in a range of scientific and medical fields, as part of the Technion’s commitment to scientific excellence and the advancement of human health.
MRI is an important technology for structural and functional imaging of tissues and internal organs including the brain, is non-invasive, and avoids exposure to ionizing radiation. According to the Center’s manager, Dr. Dafna Link-Sourani of the Faculty of Biomedical Engineering, “the MRI study is characterized by being interdisciplinary and involving various engineering faculties (electrical, computers, mechanical, and material) and sciences (physics, chemistry, and biology), and of course medical research.”
According to Prof. Moti Freiman, who is the Center’s academic director, “Many researchers at the Technion have been waiting for the arrival of this essential research tool, and until now have been using other MRI centers for their research. The device will be available to researchers from a wide range of disciplines at the Technion and will also be used by industry researchers who want to deepen their R&D. The uniqueness of the new Center is its location within an engineering faculty, in an institute which is recognized as a global leader in innovative research, with a wide range of engineering fields. This will significantly help to advance innovation at the forefront of research and technology and to develop solutions to important clinical problems. There is no doubt that Siemens is pleased to have brought us the scanner, as we hope that Technion researchers can offer significant improvements in its performance.”
The commencement of the new center’s activity, expected later this year, is the result of ongoing fundraising led by Technion management, together with several Technion researchers: Professor Shulamit Levenberg, former dean of the Faculty of Biomedical Engineering; Dr. Moti Freiman, and Dr. Firas Mawase of the Faculty of Biomedical Engineering; Professor Tzipi Horowitz-Krauss of the Faculty of Science and Technology Education, and Dr. Yoad Kenett of the Faculty of Industrial Engineering and Management.
This Center will be the first human research MRI center of its kind in the north of the country and is also set-up to explore children’s development. To that end, it includes a mock scanner, making it possible to acclimate children and infants to the imaging process prior to entering the actual device.
Israeli medical device company SoniVie, announced on Sunday that it received Investigational Device Exemption (IDE) approval from the US Food and Drug Administration for its REDUCED1 (Renal Denervation using Ultrasonic Catheter EmitteD energy) pilot study to treat resistant hypertension patients with renal artery denervation using its proprietary therapeutic intra-vascular ultra-sound system, or TIVUS.
Renal denervation with TIVUS is a minimally invasive procedure that uses high-frequency non-focused ultra-sound energy to burn away nerves in the renal artery. The TIVUS catheter is inserted into the pulmonary artery and selectively damages nerves afflicted by the disease without touching vessel walls or damaging adjacent tissues. This causes a reduction in the nerve activity, which decreases blood pressure and is meant for patients who suffer from resistant hypertension.
Resistant hypertension is defined as blood pressure that remains higher than 140/90 mmHg despite the use of three hierarchical classes of antihypertensive medications at their most appropriate tolerated doses. The condition affects millions of people around the world, increasing the risk of heart attack, stroke, and kidney failure.
Founded in 2014, SoniVie has developed a first-of-its-kind ultra-sound denervation platform with active programs establishing nuanced therapeutic solutions for pulmonary hypertension denervation, renal artery denervation for resistant hypertension, and lung denervation for obstructive pulmonary disease with chronic bronchitis.
“We are very pleased that the FDA has approved the REDUCED1 study,” said Christian Spaulding, chief marketing officer of SoniVie. “Sites initiation has started, and many clinical teams have responded very favorably about participating in the study.
“There is a significant number of patients that may benefit from our technology and we are genuinely happy for this important step towards the introduction of TIVUS in the US,” he added. “There is a lack of effective therapeutic solutions for patients suffering from resistant hypertension, and physicians are looking forward to a safe, effective and easy to use device treatment.”
“This is a significant US regulatory milestone for SoniVie, starting the feasibility study using the ultra-sound ablation platform in the US for the renal denervation indication,” said Tomaso Zambelli, CEO of SoniVie. “This is a major step and priority in the company’s history.”